SUMMARY:
A prostate needle biopsy is the only way to definitively diagnose prostate cancer, even when PSA blood tests and multiparametric MRI suggest that cancer may be present.
The article explains how biopsies are performed, compares transrectal and transperineal approaches, and reviews the three main imaging guidance methods: ultrasound, fusion MRI, and in-bore MRI.
Evidence cited by Sperling Prostate Center indicates that in-bore MRI-guided targeted biopsy offers the highest diagnostic accuracy while using fewer needles and reducing the risk of side effects.
The most effective prostate biopsy combines precise imaging with the fewest necessary tissue samples, and the article concludes that in-bore MRI-guided targeted biopsy currently provides the best balance of accuracy and safety.
What is a prostate needle biopsy?
A prostate needle biopsy is a procedure to take tissue samples out of the prostate gland in order to determine if prostate cancer is present. In fact, it is the only way to diagnose the exact cancer cells.
Before a biopsy is done, there are two main tests to determine if a biopsy is necessary. One is a blood test, the other is an imaging scan. These two tests together establish the probability that cancer is present, but they are not the same as a diagnosis. Only a biopsy can provide a diagnosis needed to plan treatment.
The Sperling Prostate Center offers pre-biopsy testing to know if a biopsy is needed. If so, the Center provides the most accurate biopsy method.
What are the two main tests to know if a biopsy is needed?
The first test is a blood test called the PSA test. PSA stands for Prostate Specific Antigen. Prostate Specific Antigen is a type of protein on the surface of prostate cells. A small amount of this protein is naturally “shed” into the bloodstream, and the blood test measures the level.
Normally, the level of PSA in the blood is low. However, if unusual activity disturbs the prostate gland, it will shed more PSA into circulation. Unusual activity can be things like an inflammation, prostate enlargement with aging, sexual activity, riding a bike, and prostate cancer. Thus, a higher-than-expected PSA level does not necessarily mean prostate cancer, but it is suspicious.
Often a doctor will order a repeat PSA blood test after several weeks. If it is still suspicious, a second test is needed to see if prostate cancer is a possible cause. It is a special type of scan called multiparametric magnetic resonance imaging, or simply multiparametric MRI.
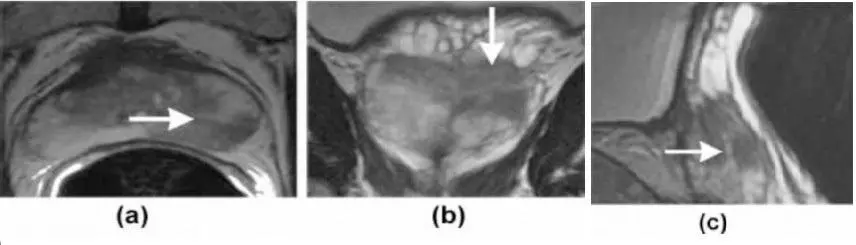
Noninvasive multiparametric MRI shows the difference between normal prostate tissue and abnormal prostate cancer. It is very good at revealing an area called a suspicious lesion. Unlike x-rays or CT scans, however, MRI does not involve radiation.
Based on the abnormal area’s characteristics, an experienced doctor looking at the images can tell if it is a condition like an inflammation or aging-related enlargement, or if the abnormality is probably cancer. If it is probably not cancer, a biopsy is not needed. In that case, going forward the PSA blood test is used for future monitoring. If PSA continues to rise, multiparametric MRI can be done again.
On the other hand, if the area is probably cancer, a needle biopsy is needed for diagnosis. Images a, b, and c below are actual MRI images. The white arrows point to suspicious lesions:
How is a biopsy done?
A biopsy involves insertion of a number of hollow needles into the prostate gland. When quickly inserted and removed, the needle captures a thread of tissue containing prostate cells. Imaging is used to guide where to place the needles. Before inserting biopsy needles, the area should be numbed to avoid pain.
As each needle is removed, the tissue specimens are placed in separate containers labeled with the precise location from which it was taken. These containers are sent to a laboratory where a specialist called a pathologist analyzes each specimen under a microscope.
If cancer is seen, its location and amount will be recorded. Most importantly, the pathologist assigns a Gleason score to each cancerous specimen. This score indicates how abnormal the cancer appears. The higher the score, the greater the aggression level.
Given the location of the prostate gland, there are two different pathways for placing biopsy needles:
- Transrectal – The biopsy is performed through the rectal wall
- Transperineal – The biopsy is performed through outer skin between the scrotum and the anus
What kind of imaging is used to guide biopsy needles?
There are three main imaging methods used today to guide placing biopsy needles.
- Transrectal ultrasound (TRUS) is live imaging used to guide either transrectal or transperineal pathway. While ultrasound shows the prostate gland as well as the insertion of needles, it does not define differences in tissue, that is, it cannot show a suspicious lesion as multiparametric MRI can. Therefore, needles are systematically mapped into sections of the gland, but the doctor can’t tell if the needles hit cancer so it’s random. This method requires a minimum of 12 needles to sample according to the “map.”
- In-bore multiparametric MRI is live imaging used to guide either transrectal or transperineal pathway. The biopsy is done in the bore (tunnel) of the magnet. Because it shows the difference in tissue characteristics, a doctor can precisely target suspicious lesions. This method uses the fewest needles, usually 2-4, because the doctor can see the lesion. It is the most accurate biopsy because the more aggressive cancer cells tend to be near the center of the lesion.
- Fusion is an imaging hybrid that merges live TRUS with previously captured still images from multiparametric MRI. Specialized software synthesizes the still MRI scans and the live ultrasound, generating a synthetic picture of the patient’s prostate showing the site of the suspicious area. This helps the doctor target the lesion, while the ultrasound shows needle placement in real time. However, the possibility of minor errors exists. Thus, it’s typical to take extra systemic samples throughout the gland to offset the chance of missing any cancer.
NOTE: Fusion-guided biopsies are often called MRI-guided biopsies because they integrate still MRI images. This can be misleading, because the MRI images are not live. Only in-bore MRI biopsies have live MRI guidance for the greatest accuracy.
Is there a “best” prostate biopsy?
Because biopsy needles are invasive, all methods have some risk, however small, of side effects:
- Infection
- Temporary blood in urine or semen
- Discomfort/pain due to inadequate numbing
Also, no biopsy method is guaranteed 100% error-free. There are error risks that can include:
- Under-detecting (missing) the more aggressive cells
- Over-detecting insignificant prostate cancer that may not require treatment
Therefore, a “best” prostate biopsy would maximize diagnostic results while using the fewest needles to minimize side effect risks. Studies have shown that transperineal biopsy pathways have significantly lower infection risks than transrectal biopsies because they do not introduce bowel bacteria into the prostate bed. Also, the fewer the needles used, and the more accurate the image guidance, the lower the risk of biopsy side effects and diagnostic error. In-bore MRI guided biopsies best fit this standard.
Dr. Dan Sperling cites a 2021 comparison study showing that in-bore biopsy “in-bore MRI-targeted prostate biopsy had a higher target-specific cancer detection rate than did fusion biopsy.”[i] Dr. Sperling notes, “True in-bore MRI-guided targeted biopsy is not as widely available as it should be. Our Center is proud to be a pioneer in ensuring that patients do not have a biopsy if they don’t need one, and if they do, they have access to the best method at our Center.”
Frequently asked questions (FAQ)
Q: My biopsy report said I have Gleason 3+4=7 prostate cancer. Should I get a second opinion?
A: National prostate cancer organizations support getting a second opinion, as it can help you understand your disease, and give you peace of mind regarding treatment options. ZeroProstateCancer says, “Your doctor shouldn’t discourage you from getting a second opinion,” and advises that you check with your insurance to find out what they cover.
Q: Where do genomic tests fit in, before or after a biopsy?
A: To some extent, it depends on your risk factors. If you have a family history of prostate, breast or ovarian cancer, a genomic test after a suspicious PSA and/or MRI can help determine if you need a biopsy. On the other hand, if you’ve already had a biopsy, a genomic test can influence how aggressive (or not) your treatment should be. Talk with your doctor about the merits of genomic testing in your case, and check with your insurance carrier.
Q: My doctor doesn’t do a transperineal biopsy, only transrectal, but I worry about infection.
A: Share your concerns with your doctor. Doctors take every precaution to prevent infection. Your doctor will prescribe a protective antibiotic course that will begin a day or two before the biopsy, as well as a bowel cleanse the night before or morning of the procedure. Your doctor may also test for specific bowel bacteria. Be sure to follow your doctor’s instructions, and report any conditions such as a urinary tract infection prior to the biopsy.
Content reviewed by Dr. Dan Sperling, M.D., DABR — updated June 2026
NOTE: This content is solely for purposes of information and does not substitute for diagnostic or medical advice. Talk to your doctor if you are experiencing pelvic pain, or have any other health concerns or questions of a personal medical nature.
References
[i] Isharwal S, Chen Y, Coakley FV. In-Bore Versus Fusion MRI-Targeted Biopsy of PI-RADS Category 4 and 5 Lesions: A Retrospective Comparative Analysis Using Propensity Score Weighting. AJR Am J Roentgenol. 2021 Nov;217(5):1123-1130.
About Dr. Dan Sperling

Dan Sperling, MD, DABR, is a board certified radiologist who is globally recognized as a leader in multiparametric MRI for the detection and diagnosis of a range of disease conditions. As Medical Director of the Sperling Prostate Center, Sperling Medical Group and Sperling Neurosurgery Associates, he and his team are on the leading edge of significant change in medical practice. He is the co-author of the new patient book Redefining Prostate Cancer, and is a contributing author on over 25 published studies. For more information, contact the Sperling Prostate Center.
